Transmasc Health 101
Last updated: 11/03/2026
a frustrating-yet-paradoxically-empowering part of transition is the opportunity to manage your own healthcare and experiment with your body as a canvas. let's learn!
Trans healthcare is notoriously poor, doled out by reluctant cistems designed to marginalise and harm service users, and discourage trans joy if they cannot prevent and discourage transition at all. The reality of being a trans person is that you will be doing the work of being your own doctor, even in the best case scenario where you can access a compassionate and informed professional promptly and without interruption.
This guide is aimed at people considering going DIY for their hormones, based on studies, community wisdom, and storing useful links I've compiled; but it's for everybody.
Index
Guidelines
How to take T
On Gel
- How do I improve my results on gel?
- If I put the gel on my dick, will it grow faster?
- Is gel effective?
- Can I self-med gel?
On Dosage
- What dose should I choose?
- What's an ester?
- What if I have to change method?
- How do I figure out how much liquid to put in the syringe?
- How often should I take my shot?
- What is a hormone sensitive person?
- On Aromatisation
- I've just had hysto
- Should I play around with my dose?
Blood Tests
- What tests do I need?
- How to correctly interpret my results?
- When should I take my bloods?
- At a glance: good blood test results
- What unit is T measured in?
- What should my T level be?
- What should my E level be?
- What about full blood count?
- What is DHT?
- What is SHBG?
Doing my Shot
- How do I do my shot?
- Should I aspirate?
- Oh god i did my shot and now there's blood everywhere
- On Bubbles
- On Leaks
- On Scars
- On Allergies
- My shot is painful
- My IM shot site is in pain but it's been a few days, and also I'm feeling cranky
On Injection Kit
- What are the basic supplies I need?
- What needle size do I choose?
- What are Luer-Lock and Luer-Slip syringes?
- What is a Low-Dead-Space Needle or Syringe?
- How do I safely use ampoules?
Medication Safety
- Should I keep it in the fridge?
- My bottle of T says for IM only??
- Can I reuse this bottle or ampoule? I didn't use the whole quantity
- Can I reuse this syringe or needle?
Life on T
- What is the history of medical T?
- What are the effects of T?
- Keep a diary
- My period hasn't stopped
- I have sex in ways that risk pregnancy - do I need birth control?
- My man cave is painful during sex/painful generally
- Can I grow a prostate on T?
- What makes fat redistribute?
- I've just started T but my face is rounder than it was and less masculine
- What impacts my results?
- What is Endocrine Dysphoria?
- Studies & Science about Testosterone
NHS Transition
Safety
Non-Hormone Tips
to add
- how do i buy bitcoin
- how can i tell a source is safe
- should i tell my doc i am DIYing
Changelog
Health Guides
Quick-Start Guide
Here is everything you need to know to get started
- Read an official health guide and decide on a starting dose
- Choose between IM and SQ injections; if you're not sure, pick SQ
- Find a source and buy hormones
- Buy supplies to inject
- After three months, do a blood test
- No fear.
Official Guidelines
For people who would like to understand the kinds of pre-treatment tests, dosing regimens etc used when taking transmasculine hormones. These are guides doctors use for learning to treat trans people.
- Primary Health Care for Trans Patients: Masculinising
- (Rainbow Health Ontario). A particular favourite. (archive link)
- Men's Health Clinic UK Blog
- A private clinic for cis men on T, with a very informative blog explaining endocrinology, testosterone, and hormone science. Fantastic resource. I've linked to their blogpost explaining their preferred T regime (archive).
- Hudson's Guide
- Community classic! Last updated 2017. (archive link)
- Practical Guidelines for Transgender Hormone Treatment
- (Boston University School of Medicine) (archive link)
- Overview of masculinizing hormone therapy
- (University of California) (archive link)
- Endocrine Management of Gender Dysphoria in Adults
- (Welsh Health Service) (archive link)
- Hormone management in Trans men
- from Trends in Urology
- Clinical practice guidelines for transsexual, transgender and gender diverse minors
- (Anales de Pediatría Vol 96, Issue 4, April 2022) (archive link)
- Anabolic Steroids: A Guide for Users & Professionals
- by Exchange Supplies
- IPED info
- (Public Health Wales)
Self Med Community
If you are thinking of managing your own healthcare, there are community-written resources on dosages and methods:
- DIYHRT.wiki
- Make this your first stop! Highly recommended!
Indviduals and groups who tweet about this and share knowledge!
- DIYHRT.github.io. Highly recommended
- @Bobposting
- @TransHarmRedux - (Ireland & Scotland)
- @TransHealthNet - (Ireland & Netherlands)
- r/TransDIY - no help for trans men provided on the reddit; but get an invite to their Discord
- r/SteroidsUK - for cis men but often has up to date source links
You can also write to the Trans Healthcare Network: transmutualaid@protonmail.com . They are mostly active in Ireland and the Netherlands, but have general expertise.
Informal places to learn about T include trans communities; testosterone replacement therapy communities for cis men; and anabolic steroid using communities for bodybuilders and athletes.
How to take T
Where do I inject T?
There are two ways of administering injectable T; and there is also gel, which you put on a muscle, but is more expensive and trickier to find.
The two methods describe where you put the needle and inject the medication. Subcutaneous or SC means 'under the fat'. Intramuscular or IM means 'into-the-muscle'.
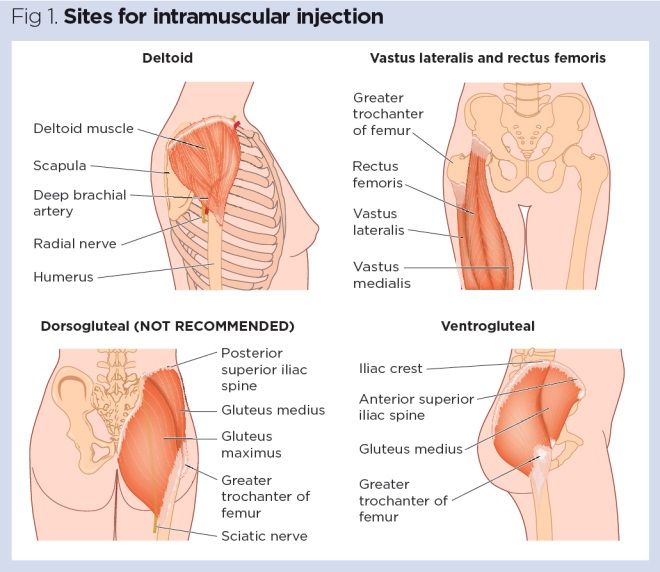
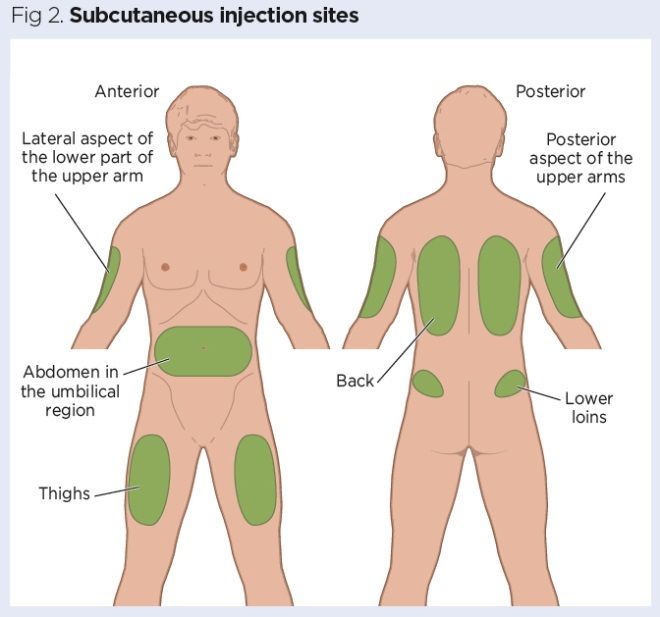
Illustrated guide to injection sites
Finding the Vastus Lateralis (it's sort of on the diagonal edge of the thigh, if that makes sense - not straight into the top, nor straight into the side, but a secret third place in-between)
Which method should I choose?
Studies demonstrate that both methods are viable, but people tend to prefer SQ. The Trans Healthcare Network seem to think that SQ is easier to do than IM and, consequently, a better option for people administering their own healthcare. For, say, a weekly 50mg injection either will work.
IM tends to be preferred for if you are injecting a large amount because it can hold more. Some T preparations will 'sit' in the muscle and disperse over a period of time (Sustanon, Nebido, i.e. things designed to work over three weeks, three months or more) and for these, IM is the correct choice.
Different T preparations come with different preferred application methods. Because of the thick gloopy carrier oil it is in, they recommend you IM Testosterone Enanthate - because it is less painful.
I find SQ less psychologically intimidating (much smaller needles, that go diagonally into the surface of the fat, instead of really long needles that go deep into the muscle) - but I have at least one friend who has the other experience, who finds the thigh you do IM with is less difficult than fatty areas like the tummy you use for SQ.
Do IM and SQ produce different results?
It depends on what you are asking
In terms of masculinisation, IM and SQ are essentially the same.
However, you may still experience them as different. Oil absorbs more slowly in fat than in muscle. Therefore, IM peaks faster and then has a more dramatic trough at the end of the week; SQ can be a smoother ride, being more consistent throughout the period.
If you are hormone sensitive, SQ is a better choice (if you have bad moodswings around your period, for example, due to the effect of hormones changing in your body). If you are at risk your T or other health markers becoming dangerously high, SQ produces less of a spike.
I first noticed this because I noticed that IM made me a lot happier than SQ, despite being on the same dose. I therfore upped my SQ dose by a tiny fraction (0.2ish), to gain the same outcome. In other words, that "peak" sensation was correct for me, and I just needed to adjust so that higher level was my baseline. The joy of self medicating is you can just do this.
The subcutaneous route allows for slower absorption compared to the intramuscular route, which in turn leads to more stable levels, decreased aromatisation of testosterone to oestrogen and less possible negative side effects.
The Men's Health Clinic
Bodybuilders who use steroids tend to believe that IM is better and SQ sucks. I believe this is purely subjective: a bodybuilder chasing a certain kind of emotional high and fast blast results will find it better with the higher spike that IM produces. Bear in mind those guys take 600 - 1000mg a week as a standard dose, for a handful of weeks and then a break; by contrast, we take 50-100mg every week, with the aim of experiencing safe stability for the rest of our lives. They're chasing intensity. And, not unlike trans men, they are also medicating anxieties around their gender - quick muscles and the sense of intense masculine drive. I believe this is causing them to discount the effecacy of SQ.
On Gel
Some people do well on gel.
I'm saying that now, because I've tried gel and I hated it. what I found was that it has a 'cycle' of a few hours and so I'd be falling into trough twice a day (most gel absorbs in the first 4 hours). It's unclear if I'd have stabilised on it if I persisted - I just got so ill I never waited to find out. I guess my skin just absorbs badly. My healthcare provider insisted that the opposite could be true: that I was absorbing so fast that it was converting to estrogen. Either could be the case: poor-absorbers and fast-hormone-responders are both kinds of people that exist.
A big issue on gel is executive function - taking it once or twice daily and then waiting around for it to dry - it's about as fast as hand sanitiser, but I'm impatient. And I have days where revealing parts of my body is too difficult.
How do I improve my results on gel?
- Rub it onto a muscle. Americans seem to do upper back and upper arms; my NHS advised the thighs (possibly because clothes prevent transferance to other people, and it's unlikely a woman will accidentally touch your naked thigh without you noticing). This study in cis men found that arms/shoulders is maximally effective.
- Other studies suggest rotating your sites is the thing to do - so your skin gets a break
- Clothes can rub it off, so leave the site open to the wind and sky for as long as you can - at least while it dries - and my dear boys, refrain from anything skintight.
- You are absorbing through the pores - so take a hot steamy shower just before, which will clean the skin of any gunk barrier and open the pores.
- Wash your hands after applying the gel, as it can transfer to others (women, children, pets, door handles) and that's bad. If you're super fuckin' broke, this means you probably shouldn't have that steamy shower in the public gym - or, if you do, be hyperthoughtful about ensuring your wash your hands in a way there's no risk to others.
- Reportedly, moisturising helps. An hour after you apply the gel, moisturise the area; the alcohol in the gel dries out your skin as it evaporates, inhibiting absorption, so moisturising re-opens the pores and increases absorption. There has been a study, but I can't seem to find it; iirc this improves absorption by around 18%.
- Most gel is absorbed in the first 4 hours, so wait at least 2 hours until after applying gel before going for a swim etc; the study also shows that showering 6 hours after gel inhibits its effectiveness, but 10 hours afer is fine.
- You may be able to see why I hate gel: applying it correctly is a full time job, and I have ADHD
Should you put all your gel on one area, or across four areas? Both are effective. I can't quite follow the argument of this study, which seems to conclude that both methods are basically the same, but also that over 4 areas increases DHT and possibly T as well. See what you make of it.
If I put the gel on my dick, will it grow faster?
The standard T gel you get for transitioning with is not location-based, i.e. it will not cause more T Effects on the place its put on the body. The gel is alcohol based - it stings, it dries you out, you don't want it on your sensitive bits.
What you're thinking of is a topical DHT cream - discussed below, but typically very hard to get your hands on even legally
Is gel effective?
Definitely for some people. Here's one study on monitoring the results of gel - 70% found it effective within two hours, but only 30% had adequate serum T after 23 hours.
However, it definitely seems pretty common that gel is ineffective for some people (ineffective defined here as, the person isn't meeting their transition goals with it, whatever those are). No way of knowing why this is or if you'll be one of them.
Can I self-med gel?
I hate gel (except as a recreational horny euphoriant) so I've never tried. What I've always heard is that gel is hard to find, and disproportionately expensive. Additionally, cis male steroid users believe it is less effective than injections, so there's less of a market for it. But if you prefer gel for any reason, do your own research on this.
On Dosage
What dose should I choose?
Look at the health guides!
The 'male range' for T is actually really large. 'More' does not mean faster, manlier, or more serious: it's very individual what the right point is for you, and some people get very intense changes on low doses where others will need more for the same effect. I make my guide that right is when I feel good.
Additionally, different people respond to the same dose in different ways. Suppose you take 1 pump of gel, and Aiden takes 4 - you could have an identical blood result for how much T is in your body; and if you and Aiden both have blood testosterone of 400, you might feel dandy and he might feel like death. Or you might be masculinising at the same rate, but that meets his goals for transition but not yours. It's a tinkering process to get this where you want it.
What's an ester?
Pure T gets used immediately by the body. Different esters of T break down and release at different speeds.
T Cypionate, T Undecanoate etc are all the names of different esters. This gives you a clue as to how frequently that form of T needs to be taken. The speed a chemical breaks down is called half-life (the amount of time it takes for half the remaining substance to go - so it's a graph, not an absolute number.)
Sustanon contains several esters, because it's for three weeks so it needs some T that works immediately and some which persists.
- T gel: unknown, is it even in an ester? It's fast! Feels like 4 hours
- Testosterone Enanthate: 4.5 days
- Testosterone Cypionate: 5.0 days
- Testosterone Undecanoate: 20.9 days (Nebido)
You can use this information to approximately plot how each version releases into the body. That won't tell you anything about how much T will appear on a blood test, or how it will impact you as an individual; but it can be useful to compare if you're swapping methods - finding out what the points you felt well or bad were in actual terms, and seeing how to replicate or reduce them.
What if I have to change method?
'Translating' doses between T methods are hard, because each one functions slightly differently. If you swap methods, you may need to re-learn your dose.
However, understanding how each method works and learning more about how your body responds to T can help you draw some inferences.
I have found one NHS resource with information on how to approximately swap between doses of substances commonly used on the NHS:
- Sustanon (250mg intramuscular injection every 28 days) = Testogel pump 2 squirts (40.5mg) or Tostran gel 4 squirts (40mg)
- Sustanon = Nebido as per loading protoco
- Nebido switch to Sustanon or gel = wait until testosterone level falls below 15 nmol/L and then start either Sustanon 250mg every 21 days, or Testogel pump 2 squirts per day, or Tostran 2% gel 4 squirts per day
How do I figure out how much liquid to put in the syringe?
(this section quoted directly from DIY.HRT wiki, as my own arithmatic is too poor for me to safely summarise)
Vials of testosterone are usually compounded at either 200mg/mL, 250mg/mL or 300mg/mL. This means that for a 200mg/mL vial, every 1mL of liquid will contain 200mg of testosterone. A 10mL vial will then contain a total of 2000mg of testosterone.
The formula to calculate how much liquid to inject is:
(amount you want to inject) ÷ (concentration of the vial)
= amount to inject per dose in mL
- If you wanted to inject 20mg and you have a 200mg/mL vial,
- 20 ÷ 200 = 0.1
- 0.1mL per injection
- If you wanted to inject 50mg, and you have a 200mg/mL vial,
- 50 ÷ 200 = 0.25
- 0.25mL per injection
- If you wanted to inject 100mg and you have a 200mg/mL vial,
- 100 ÷ 200 = 0.5
- 0.5mL per injection
- If you wanted to inject 50mg and you have a 250mg/mL vial,
- 50 ÷ 250 = 0.2
- 0.2mL per injection
- If you wanted to inject 50mg and you have a 300mg/mL vial,
- 50 ÷ 300 = 0.17
- 0.17mL per injection
How often should I take my shot?
T is used by the body slowly after you take it, and it'll be a bit individual how long it takes to be used up. You will feel a lot of T at the beginning of the cycle, and very little towards the end.
If your T isn't feeling good across the whole week, your first instinct might be to increase how much you're taking. But no matter how much you take, it'll exit the body on the same schedule - so all you've really done is increased your swing between high and low. Cycles that overlap at the end and beginning prevent you going into that low-T depression, and reduce the impact of change if you are hormone sensitive.

If you are adjusting your dose frequency by more than a day or two, and/or if the current level of T you are on is moderate or high - consider splitting your dose. For example, instead of 50mg once a week, do 25mg every 4 days. Because T stays in the body for a while after you take it, taking 50mg every four days would to result in a far higher level of overall T at any one time. That makes what you've done an increased my dose intervention, not a adjusted my cycle intervention. You may want or need both, but ensure you don't do it accidentally
I'm especially interested in this microdosing protocol at the moment, which seems like a smart way to get a stable dose without big spikes and drops. Notice that in this article, he describes three doctor-recommended ways of taking testosterone enanthate:
- 12.5mg every day
- 50mg every 3.5 days
- 250mg every 2 - 3 weeks
All of these put similar amounts of T into your system for a similar period of time, but the experience of cycling on and off differs. This likely won't impact your pace of masculinisation (but it may!) but it likely will impact your emotions.
What is a hormone sensitive person?
Some people are more sensitive to hormonal change. Indicators include having had bad PMDD before transition, or experiencing dramatic mood and dysphoria swings at the end of T cycles. Here's a study:
the evidence we present shows a recurring pattern of hormonal sensitivity at predictable but different times across the lifespan of some women (i.e., menarche, the premenstrual phase, hormonal contraceptive use, pregnancy, the postpartum period, and menopause). These findings provide support for the hypothesis that there is a subgroup of women who are more susceptible to physical, psychological, and sexual symptoms related to hormonal shifts or abrupt hormonal fluctuations that occur throughout the reproductive lifespan. We propose that this pattern reflects a Hormonal Sensitivity Syndrome.
The hormonal sensitivity hypothesis: A review and new findings
Sensitivity to hormones kicks in most strongly, of course, when you begin T - but I'm mostly not talking about 'teen puberty' symptoms like moodiness, libido and acne, which hits everyone. I'm discussing something more subtle, similar to the imperceptible horror of living within a menstrual cycle which one cannot see outside of, living each moment as if it were your authentic self, feeling that self shift on a predictable calendar, and feeling each new self is equally true in turn.
What this feels like for me on T is when I reach the half-life point of my medicine, it's like dropping off a cliff and I come to bits. It is extremely marked. Other experiences I've had which I believe represent hormone sensitivity include:
- Extreme PMDD before transition
- feeling the difference between the same dose with IM vs SQ (despite the popular belief that they are identical)
- feeling the difference between the same dose on TE and TC (ditto)
- not being able to tolerate gel because the half life is so short and the mood swings so frightening
- becoming dysphoric in cold weather on long-acting hormones because the carrier oil slowed down in my body.
If you are hormone sensitive, look at some of the options for tinkering explored on this page. A slower-release testosterone, swapping from IM to SQ, increasing shot frequency while reducing the dose, or some combination
On Aromatisation
In cis men, some testosterone is converted back into estrogen. This is a natural regulating process to accomplish balance. When cis men take TRT or bodybuilding steroids, if they take too much there is a risk their estrogen will become too high - leading to gynomastica and other issues. However, cis men do need some estrogen to remain healthy. The normal range for adult man is 10 – 40 pg/ml (according to Mayo Medical Labs; for women is 15 – 350 pg/ml)
Broadly, the same things are true for us. Taking T can put us at risk of both too-high and too-low estrogen levels and, intuitively, I believe we should be aiming for the correct estrogen range just as we do for the correct testosterone range. If you take too much it'll turn back into E
is a transmasculine old wives tale as we police one another's behaviour; but two studies done on this topic have revealed no evidence of this happening in trans men. Though never say never: it's theoretically possible.
On the whole, however, it probably isn't happening, and there should be no need for estrogen blockers. However, such a thing does exist if you need to look into it!
I've just had hysto
Community wisdom is that commonly, you (can? should?) reduce your dose after hysto. Removing the uterus changes the whole hormonal context for your body and therefore, you may need to review your hrt plan.
There's anecdotal evidence of trans men continuing to experience a period cycle in their moods, despite no longer bleeding or experiencing pain.
Should I play around with my dose?
Absolutely. Life is short, and it's your body.
In general, there's no fear to be had of taking less or more infrequently, so be wild and free with that; but any time you're taking more or more often be cautious and methodical and go very gradually.
You can definitely do yourself serious harm with T, so don't go outside the parameters rashly. Damage such as polyctheimia has no symptoms the patient experiences, so you won't necessarily feel you're in the red zone without blood monitoring. And dangerously high T can feel great, I mean really great - that's why it's a popular lifestyle drug! - and that can make reconciling yourself to a safer dose extremely tough.
Your need to go up may be authentic and therefore doing it is a health need, and remaining where you are the danger: do not be afraid. But don't be rash or do a big jump.
Blood Tests
What Tests Do I Need?
On the NHS, it is standard to get your baseline bloods taken before you begin; once you begin on HRT, it is impossible to recover this baseline data. However: in America, its not standard to get a pre-T blood test at all, so if you're on a budget it evidently isn't that important.
I've discussed this with friends, and we decided that the NHS are being thorough and it's a reflection of a patrician attitude, whereas in the USA - because people are paying their own way - there's more of a culture of only doing what's actually needed.
The NHS test should measure:
- Full blood count (FBC)/Complete Blood Count (CBC)
- liver function test (LFT)
- HbA1c*
- fasting lipids
- prolactin
- luteinising hormone (LH)
- follicle-stimulating hormone (FSH)
- testosterone
- estradiol
- sex hormone-binding globulin (SHBG)
- vitamin D.
- Renal function if indicated.
This Body Transformation Test - a mail-order test which covers all the bloods taken by the Welsh Health Board - I suspect, tho they did not say this on the website, the target market is trans people.
Getting regular blood tests is essential to safe T use, and that's even more true if you are accessing your medication from a questionable source. 3 months and 6 months is the standard pattern on the NHS.
In the UK, routine blood tests will check your testosterone only. In other countries, it checks your T and E levels. In my opinion, you should test for both - so you have more data about what your body is doing. UK monitoring checks test for:
- FBC (full blood count)
- LFT (liver function test)
- fasting lipids
- testosterone
How to correctly interpret my results?
A common issue with getting blood tests done is, the service will assess if your bloods are 'correct' based in part on your expected gender, and not document that this is a trans person's blood test which needs interpreting in that light. I believe you want the blood test to be done 'as a man' to check T is in a ''male range'', and so it doesn't come back interpreted as if you were a woman. The same is true when checking your Full Blood Count: they should be looking at male reference ranges, not female ones. If you're nonbinary, then consider your goals and ask your provider to assess the bloods in that context. An effective health service should be able to record that you are trans, and therefore interpret the results in that light, however I've yet to hear of an effective health service except in long-lost legends of ancient days.
To combat this issue, verbally instruct your healthcare person to assess your blood in the male range when you have the blood taken and when the blood test is booked. When your results come back, double check your own levels against reference ranges online.
When should I take my bloods?
Big shrug. No one knows, no one has cared enough to come up with a good answer. How to assess testosterone replacement therapy correctly is a contested question in the field, as your T fluctuates across the cycle. Take it at the same time for every reading, so you can compare them.
On the NHS, they take the morning of your shot, and the day after, to establish your absolute highest and lowest readings. This seems wise!
At a glance: a good blood test?
Each of these are explored more below, but the target range for cis men is:
- testosterone: 300 - 1000ng/dl / 10.41 - 34.7nmol/L
- hematocrit: 54% or less
- estradiol: 10 – 40 pg/ml
What unit is T measured in?
ng/dL or nmol/L. Here's a converter to turn one unit into the other. For your curiosity:
- nmol/L = nanomoles per Liter
- ng/dL = nanograms per decilitre
What should my T reading be?
The Endocrine Society’s 2017 clinical guidelines for transgender HRT recommend that trans men maintain “testosterone levels in the physiologic normal male range”, a range which is given as 400–700 ng/dL. On trans community sites, 300-1000 is often cited.
Zinnia Jones has a very interesting article querying these numbers. She cites a study which revealed half of trans men have readings outside that range. Additionally, there are several other proposals for what the "normal male range" is, a far wider span of 210 - 1510. Finally, she notes the difficulty of getting an accurate T reading by blood tests because T fluctuates so much. Endocrinology, a textbook by J. Larry Jameson, MD, PhD, Leslie J. De Groot, MD, is critical about the effectiveness of current T measuring techniques, describing current techniques as an 'unproved theory'.
All this is to say that T levels are one part of a complete picture. How you feel, if you're happy with the rate of change, and what your danger markers are looking like, are as important than an T reading when assessing your situation.
See also: What are Normal Male Testosterone Levels? from Optimale
What should my E reading be?
Not everywhere tests E, relying instead on menstruation stopping as a sign for low enough
. According to Mayo Medical Labs:
- The normal range for adult man is 10 – 40 pg/ml
- For women is 15 – 350 pg/ml.
One study showed that for trans men, estradiol levels were observed to decrease from an average of 81 pg/mL at baseline to a steady average of 54 pg/mL during treatment. In other words, it is good to aim for a cis male range estrogen level, however it's normal for our readings to remain a little higher.
What about my Full Blood Count?
"Polycythemia is defined as serum hematocrit (Hct) or hemoglobin (HgB) exceeding normal ranges expected for age and sex, typically Hct > 49% in healthy adult men and >48% in women, or HgB >16.5g/dL in men or >16.0g/dL in women." - see wikipedia.
The blood is made up of plasma (watery stuff) and red blood cells (solid stuff). Taking testosterone increases the number of red blood cells, which is good for athletes - more oxygen can be carried to muscles faster - but too much, and the blood gets sludgy. This leads to an increased risk of blood clots and heart attacks.
Taking high levels of testoterone raise the risk of high hematocrit. Typically, trans men have a higher hematocrit level than cis men. The risk is greater when using short-acting esters (like cypionate or enanthate) because of the way they work: on the day of your weekly or biweekly shot, the level of T in your body is 'supraphysiological' - i.e. higher than biologically normal or possible. That is more likely to put you into the zone for dangerous outcomes. You won't necessarily have physical symptoms when your hematocrit is too high: that's why the blood tests are important.
The hematocrit reference range for men is 42% to 50%. I've also seen 54% listed in some sources; on the NHS, I've been told it's 52%. Bodies are not machines, but you can see the ballpark range for what 'too high' is going to look like.
The first line treatment for high hematocrit is just to take less T. It's hard to know if this is genuinely the only option, or reflective of a transphobic medical culture where our testosterone use is seen as inherently cosmetic and risky. Cis men with high hematocrit are not prescribed T blockers, because the impact on their body image and mood would obviously be unacceptable.
Blokes who do TRT talk about giving blood as a way to reduce their hematocrit levels informally. In an medieval way, phlebotomy - bloodletting - is recognised as a treatment for high hematocrit. One study looking at this discovered that levels don't go down in TRT users as much as they might hope or assume; whereas this study noticed a stronger effect. I've also been told about phlebotomy as an option by an NHS doctor.
Other options include swapping to a longer-acting formula (apparently, undecanoate doesn't raise levels so much as cypionate and enanthate), microdosing (taking far smaller amounts each day), or some other combination of a different type of T and a different frequency.
What is DHT?
In the body, testosterone you take turns into other chemicals. One is DHT. DHT is associated with bottom growth, body hair growth, prostate growth but also head hair loss. It also plays a role in mood and increases libido.
Finasteride is a DHT blocker which some transmascs choose to take, to change their outcomes on T (for example, if you want to avoid one or more of the results of DHT). See the section on hair loss below. I also wrote a trip report of my experience of trying finasteride.
As a medication, DHT is referred to as androstanolone or as stanolone. There are pervasive online rumours that DHT in a cream mixed by a compounding pharmacy can be put on your junk to boost bottom growth. This works for cis boys with intersex conditions. There is no studies on whether it will work for us, and this cream is very hard to access depending on where you live. See below
What is SHBG?
Quoted from a cis men TRT conversation because it interested me:
SHBG stands for sex hormone binding globulin. It's a protein made by the liver and attaches itself to sex hormones found in both men and women. These hormones are: Testosterone, the main sex hormone in men. Dihydrotestosterone (DHT), another male sex hormone. The more SHBG you have, the more testosterone is 'stolen' and is unavailable to be used by the body. So you could have a really high testosterone reading but if SHBG is also high, you may experience the symptoms of low testosterone
Cis men interested in their own hormones often have very deep dysphoria brainworms, a way of talking about their bodies and internals that seem to me a deeply unmet need turning into an obsession that is hurting them. I feel a lot of affinity with these guys, but I also think their hormone science can be a little sketchy. Still, at least they're thinking about it.
Doing My Shot
How do I do my shot?
Youtube has excellent revision videos for nurses in training to emulate professional-level skills
- Introduction to Ampules and Vials - University of Manitoba Nursing Skills
- Intramuscular Injection
- 📑 How do I administer Sustanon - from Gender GP; intermuscular.
- Introduction & Subcutanous Injection Training
- How to Give Yourself a SQ Injection - Planned Parenthood
- 📑 How to Open an Ampoule
- Slow motion of an ampoule snapping
- Draw from ampule
Should I aspirate?
'Aspirating' is - you put the needle into your body, but before you inject, you then draw back the needle a tiny bit. If the syringe floods with blood, you've hit a vein or artery. You should remove the needle at once and do NOT inject - discard everything, start again. Putting substances into the bloodstream is very dangerous and this is true of T which you do not want in the blood but in either a muscle or fat.
Apparently, it's no longer recommended to aspirate for either SQ or IM injections. I suppose the logic is that if you're following instructions correctly for administration and location, there's no veins or arteries in those areas so you're unlikely to hit them (there are no veins or arteries in the skin or muscle, I guess?)
But if you're doing it right
is a bigger if
for an amateur. I always aspirate for IM, and prefer to for SQ - there's no reason not to, IMO.
Oh god i did my shot and now there's blood everywhere
Don't worry! That's fine, you're not in danger, it's normal. I'm told this is the answer. I will never believe it. Press the site with tissue or gauze; pop a little plaster on it; wash your hands because blood can carry infections; and then give yourself a little treat for being brave.
On Bubbles
You may have heard that injecting air bubbles is very dangerous. This advice is for intravenous (into-the-vein) drug users. T goes into either the muscle or skin - i.e. not into-the-vein.
That said, you do want to avoid massive bubbles if you can. Don't shake the bottle, warm up the T bottle before you start (between your hands or dip it in warm water), go slowly with drawing up (T is gloopy), repeating if you got a big bubble, and then knock any tiny bubbles you have to the plunger-end of the shot before you take it.
On Leaks
After you do your shot, sometimes T will leak out onto your skin.
This isn't the end of the world, but it also isn't ideal. Some options include:
- When you do your shot, make sure the skin dimples by about 1/2 an inch, pressing further inward with the plastic of the syringe. That way, when you withdraw the syringe, medicine wishing to escape has further to travel.
- After you finish injecting, count to 30 before removing the syringe from your body. That gives it more time to disperse
- Learn the z-track technique.
On Scars
Scars will build up in your tissue over time if you inject a lot, making it more painful. To reduce this from happening, rotate your shot site, and after taking your shot, massage the site to prevent scar tissue building up.
I've since heard this is no longer recommended, and massaging the area can make the risk of scarring worse. I need to check in with where I heard that. If you're interested, do your own research
There's now a hard lump under the skin on my favourite injection site, although it's not really dangerous, it's just there. Also, more hair growth there than on the opposite side of my body, which might be the result of microabrasions triggering hair growth - the same way a dermaroller works.
On Allergies
Your testosterone is put into a substance which then travels around the body. Different T preparations use different substances
You may be allergic to this - it could cause itching or pain at the site or, if your allergy is serious, actual danger.
Here's common carrier oils, but check your preparation before you take it to make absolutely sure: olive oil, castor oil, peanut oil, cottonseed oil, alcohol.
The most common carrier oil used by underground labs who produce testosterone on the sly and sell it by means unseen is MCT, a kind of coconut fat. I wonder if it's therefore a potential risk to anyone with a coconut allergy. MCT has a texture unlike other oils testoterone comes in, it's waterlike and not goopy and thick.
My shot is painful
Slow down. T is put in slow-moving oils. If you experience pain during your shot, and with that fear, your instinct is to speed up and get it done. Pause, and breathe. The liquid you've already injected has to disperse so give it a moment. Then continue, injecting slowly.
As discussed below, the oil T comes in is affected by temperature. If it's cold, it will move more slowly and be painful. Testosterone Enanthate, being thicker, is inherently trickier to handle. The fix is to warm the bottle between your hands or dip it in warmish water before doing your shot.
A third option is that you are allergic to the carrier oil. T is in different oils - peanut, sesame, cottonseed, olive. You may be able to swap to a different oil or T preparation.
My IM shot site is in pain but it's been a few days, and also I'm feeling cranky
Charmingly, my weatherwitch friend, IM shots will act as a kind of barometer. The liquid sits in the muscle, and disperses slowly. It's heat sensitive, and moves faster when it's warm (one reason not to store your T in the fridge, or to let it warm up to room temperature or roll the bottle between your hands before use).
If your IM site is painful out of the blue, you're feeling unexpectedly dysphoric, and the sky is ponderous and grim, you're probably sensing the coming storm. Try thermals, or a hot water bottle on the site.
(Coming back to this essay to update it, I'm really struck by my comment that experiencing painful shot sites made me dysphoric - presumably, if the liquid flows more slowly and therefore the amount I'm getting is reduced? That could be bollocks. But what I've observed is I am very sensitive to fluctuations in my hormones where most people describe no impact, so...)
Life on T
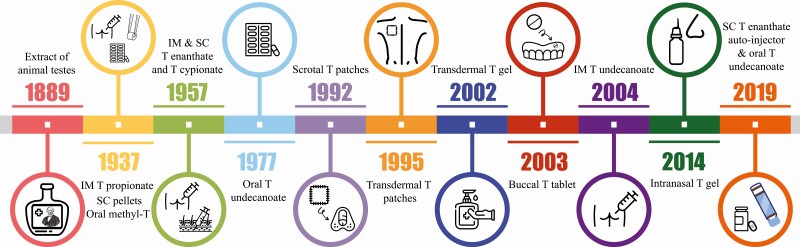
What is the history of medical T?
What are the effects of T?
HOT MEN.
Please visit genderdysphoria.fyi for a good community-run description.
Keep a diary
If something becomes difficult in your transition in future, you might need to look back and point at what exactly you were experiencing at what dose. Or, you may want to observe what your week 1, week 2, week 3 symptoms are in case you go off and on T again. You may want to identify what happens when your level is low, vs when it is high, so you can choose which you want more of. And so on.
Useful things to document:
- What dose you have taken, of what substance, on what day
- any feelings, changes, observations or experiences each day
The diary doesn't have to be attractive or in public.
One downside of doing this is you end up hyper-focused on your transition rather than living your life and letting hormones work their leaden-footed magic. In some ways, this level of focus is bad for your wellbeing and will bite you. But documenting what is and isn't working might help you get closer to the best cycle possible.
The main thing I've observed is that when my hormones are correct, I stop updating the hormone diary. I'm just getting on with life and not even thinking about it. When I'm noticing hormone-related symptoms all the time and writing them down, I know something is wonky.
My period hasn't stopped
On the NHS, the period stopping is their sign that your T levels are not too low. You might need to increase your dose
If you're unusual or unlucky, you can go on a non-hormonal birth control stop it - this is outside my expertise. Ask around in the community.
I have sex in ways that risk pregnancy - do I need birth control?
Yes. Testosterone does not work as birth control.
If your fertility is important to you, you need to address that before starting T - there's evidence that you can stop T and get pregnant, but it's also not a guarantee. This is outside my expertise also. Ask around the community for what other people do.
My man cave is painful during sex/painful generally
This can happen after a while on T. Look up 'vaginal atrophy'. There are moisturising creams available to relieve pain.
Can I grow a prostate on T?
Oh yes you can, my friend
Rather like other parts of the body, AFAB people have a Skene's Gland which is formed from the same root as AMAB people with prostates, and has also been theorised as the source of 'female ejaculation'. One study has shown that people on T can grow prostate glands inside the vaginal canal.
Anecdotally, people in phallo communities often report bottoming for anal sex feels better post-vaginectomy (that is, after having your man cave removed). This may be to do with how the angles and tissue get shunted about, or it might be due to greater comfort while naked and sexual, or both.
What makes fat redistribute?
Reportedly, the fat doesn't just move. Instead, what happens is when you lose weight the fat goes away, and when you gain it it is gained in new places.
In other words, exercise will help the process along.
I've just started T but my face is rounder than it was and less masculine
That's 'water retention'. There was an excellent post on reddit explaining this, and I can't find it. The community wisdom is that drinking more water (and reducing your salt intake) gets you through this phase quicker. Cis men taking testosterone also experience this.
What impacts my results?
There's no research on this, so the ideas put about by the community are good sense guesses. Some factors include:
- Genetics (what do men in your family look like?)
- How fast your body metabolises T (a little goes a long way for some people; how fast is it used up, how high does your dose spike)
- How much you take
- How frequently you take it
- What variant of T and method you take it with (some people are more impacted by this than others)
- How long you've been on T (some things develop and richen over time)
- How spikey your method is (peaks and troughs vs smooth sailing, and how you personally feel about this experience)
Whenever someone writes their transition is going 'badly', the community tends to reassure them that everyone's transition proceeds at a different pace, and it's just genetics and luck and time. I don't believe this. I think a lot of trans people are being incorrectly dosed by doctors who view trans people's genders and bodies as inherently different from cis people's, and that we just don't have the studies for well-intentioned doctors to get the dose correct. It turns into a self-perpetuating myth: someone having a subpar experience is reassured it is normal, and so they persist with it.
if your transition isn't doing what you want it to do, change the kind of T you take; change your dose; change your shot frequency.
What is Endocrine Dysphoria?
Based on my experience, I strongly believe there is a subtype of dysphoria mostly centered around hormonal imbalance. This may-or-may-not be the same as other trans people in a biological sense, although politically we are all bound together regardless of whence our dysphoria stems.
Ahead of writing my own thing, here's some writing about it proposing the term Biochemical Dysphoria
This might be related to the proposed hormone sensitive person - studies suggest that some people are disproportionately affected by small changes in hormonal state. It might also have overlaps with PMDD. We have no way of knowing because studies on transness are so dominated by cisgender priorities.
NHS Transition
Assorted links and resources as I find them
- A bridging prescription: your GP will give you hormones while you're on the waiting list for a gender dysphoria diagnosis. Good luck babe at getting one of these. Resources for asking for a bridging prescription, from Genderkit and TransActual
- A guide to your rights if if your GP stops or refuses care
Medication Safety
Should I keep it in the fridge?
No, not if it's oil-based. If the oil is cold, it'll flow more slowly - which will be more painful and take longer. It should be room temperature. Holding the vial or ampoule in a closed hand for a few minutes or by holding under a tap of warm NOT hot water can help, say if your house tends to be cold.
Some kinds of testosterone flows more slowly and is thicker than others - it depends on the carrier oil. If it's thick, warming it up every time is a good idea.
My bottle of T says for IM only??
I've been told by several sources that the little bottles of T which say "for intramuscular injection only" can, in fact, be used for SQ as well; and my results with this have been good.
Can I reuse this bottle or ampoule? I didn't use the whole quantity
If it's a multi-dose vial
then yes; the standard treatment in the US is to give you one little bottle for like eight months or so. This is judged sufficiently safe - the piercing in the rubber lid isn't entirely sterile and, over time, little bits of rubber/metal/grit will appear in the T and you'll have to try and dodge them and hope the injection needles are small enough to filter it out. By the end of my last prescription of this I was getting very uncomfy and wishing I could get a new prescription. Opened preparations of T will go off, gradually losing potency and potentially becoming nasty; I've heard 28 days, but that seems to be like the Best Before
labels on food at the store because, again, these multi-dose vials are the norm in the USA. But American healthcare is notoriously shit so...
Using a separate drawing up needle than injection needle as part of your routine likely increases the safety here (esp if you're sharing your prescription with a boyfriend), because the needle touching the liquid will always be maximally sterile.
In short: if it's a multi-dose vial, use it for multi-doses. But if it changes colour, has been open for over a year, is past the expiry date on the bottle, or you can see stuff floating in it, get a new one if you possibly can.
If the bottle is marked single dose
it won't have been designed with preservatives or bottle-features to keep the medication sterile. If it's a single-use glass ampoule with a snappable neck, you cannot use it more than once. Many people in the bodybuilding and diabetic community advocate drawing up all the medication into syringes and then leaving the needle and needlecap on until you need them; this seems to be wildly unsafe. The only reason why these people say you can is desperation - a system which deliberately creates medical poverty for disabled people and creates a black market forces these kinds of desperate choices and makes them very, very tempting. Avoid it, little one. We need you in future.
If you have no other option than to reuse single dose vials, get a reusable glass syringe with a lid that is designed to be sterilised and reused.
Can I reuse this syringe or needle?
Duckie, no. Discord me and I will send you some money. Or, approach your local needle exchange, trans mutual aid, or anarchist collective for some cash. This equipment is extremely cheap, and so no matter how dire your straits, you will be able to find someone with good in their heart to mail you some money or kit (in the UK, under the Misuse of Drugs act 1971, it is not an offense to supply needles and syringes)
On Injection Kit
What are the basic supplies I need?
Equipment used in the Polyclinic Video, recommended above
| Product | Quantity |
|---|---|
| 1ML Luer Lock Syringe | One per injection |
| Drawing up Needle - Sharp
Luer Lock | 18G gauge | 1 1/2" long |
One per injection |
| Injection Needle
Differs based on method! |
One per injection |
| Alcohol swabs | Six per injection |
| Small Plasters | Optional/one per injection |
| Sharps Container | Lasts forever |
PLUS an Injection Needle. Make sure it fits your selected syringe:
| Method | Gauge (thickness) | Length |
|---|---|---|
| SQ | 25G -30G | 1/2" - 5/8" |
| IM | 23-25G | 1" - 1 1/2" |
I think Exchange Supplies is cool - a social enterprise that's been running since the ~2000s with a mission of harm reduction for people who use injectable drugs (including those who do so illegally), and ships worldwide. You may be able to find a needle exchange, a trans mutual aid group, an lgbt or sexual health clinic that might help you access equipment for free if you are in need.
Here are Needle exchanges in the UK - but be aware any service run by the state is going to put you on a list Somewhere, and it may liase with police, trans healthcare systems, other healthcare systems, the welfare office, and so forth. Look for needle exchanges run by actual anarchists if at all possible.
What needle size do I choose?
The bigger the gauge number = the smaller the needle. Reportedly, the chart above is for these SQ and IM injections period rather than just for T specifically. Bigger needles, the medication will move faster (and T is an oil, so it is quite slow) - but may hurt more.
In a pinch, any needle will do: these are just the ideal ranges.
What are Luer-Lock and Luer-Slip syringes?
The Polyclinic video recommends the Luer Lock system of syringes because it ensures the needle "locks" firmly onto the syringe, with a twist. Luer Slip needles just slip straight onto the end. Some needles and syringes are one or the other, and some are both: ensure yours is a match. I've done ok with either.
What is a Low-Dead-Space Needle or Syringe?
Look out for needles advertised as "low dead space": these enable you to get more doses out of multi-dose bottles, and may reduce the risk of bloodborne disease (HIV, Hepatitus etc) if you are sharing needles with others (which - to clarify - you should definitely never do, if you can possibly help it).
How do I safely use ampoules?
If you're using snappable glass ampoules, you want filter needles for drawing up with. This is because ampoules will occasionally shed tiny bits of glass into the medication. Fucking yikes, what a godawful design. I was in two minds about the necessity of this - after all, it seems like people pretty widely use normal needles and are fine - but I changed my mind after viewing this this video. Those little shards going everywhere are substantial enough to see, and not using a filter needle is reason enough to fail nursing school.
(but not in the UK, apparently. To show good faith, I agreed to an appointment with the nurse to show me how to inject correctly, despite having already been doing so for some time. I asked about filter needles, and the nurse said not to bother.)
Ampoule-snapping is terrifying the first time you do it, and you can potentially get glass in your thumb or spattered about your space, as well as just shattering your precious bottle. You can buy an Amp Snapper for next to nothing, which will safely and effectively help with all that. In real medical contexts, they advise you throw the snapper away after 1 use (i.e. to prevent cross-contamination) but exchange supplies notes they are good for around 100 uses, so i'm sure if it's just you and the same substance the safety of reuse is tolerable.
If you don't have a snapper, you need a 2x2 gauze pad or just some gauze, and preferably, gloves, because you are about to snap glass.
Before opening the ampoule, rock it side to side and see if there is any T in the top of the vial - the bit you are going to snap off. That's wasteful. Hold the bottle gently on its side, and tip delicately, allowing the air bubble to slowly ooze into the lid and the medicine to slowly ooze into the main part of the bottle. Warming the bottle up, between your hands or dipping it in warm water, may help this process.
Is self-medicating safe?
Yes and no. There are four main concerns:
- police
- safe supply
- gender clinic responses
- your ability to treat yourself
the Law
T is used as a performance enhancement drug by athletes, hence it tends to be slightly illegal the world over. Check your local context to find out how illegal it is, and what the consquences of using it might be. Typically, your risk as a user is very low. Law enforcement targets and prosecutes dealers and manufacturers, and relies on fear of arrest to police the rest. However, the risk isn't zero - so you should take sensible precautions like, say, not carrying your meds with you in the car in a way that's visible.
Supply
Trans women who self-medicate are, basically, misusing birth control and menopause pills. These can be bought over the counter in many countries, and are rarely illegal. Unfortunately for us, we are typically buying something that was cooked up in a basement. It may or may not be horse piss, and manufacturers may or may not have followed medical cleanliness best-practice. In this, we are in the same boat as other drug users who are put into unecessary extra danger (from police and to our health) by criminalisation and stigmatisation.
One study done in the Netherlands found that 50-60% of steroids bought on the black market are dodgy: too much or too little of real medicine in the substance, bulked out with random shit, actively dangerous, or containing nothing of value at all. People do die from this, and it sucks; I enjoyed Reggie Yates documentary on cis men in the UK with body image problems, seeing a lot of overlap in needs, but it includes people who became ill or died as a result of their medical choices and it's hard to know if this was cis men dosing unwisely or dangers in the supply itself.
There isn't an easy way for everyday users to test their drugs to assess whether they are of good quality or not (as is the case with some substances). Trans Harm Network have recently bought equipment to evaluate drugs from popular self-med sources and find out more about which are safer! You can also buy steroid test kits, which will test for the presence of your desired medication; other medications; and adulterants (i.e. stuff you don't want). But the catch is, you're buying those tests from the same grey market websites that you're buying the meds from - so the problem of trust and faulty products is identical
The website eroids is a community crowdsourced list of reviews of products from other users (but with advances in AI, it's perhaps tricky to be sure if such sites contain real reviews). Traditionally, you make some buddies at the gym and find out who they rely on. Friends, cis or trans, might have a legitimate prescription they can split with you; you should hold these people dear.
Gender Clinics
Those fuckers. In some countries, self-medicating might make "official" gender care sources unwilling to work with you in future (the Nethelands, apparently). In others, self-medicating can reportedly encourage real doctors to start you on hormones as a harm reduction measure (supposedly, the UK)
But there's a harm reduction angle here where, anti-drug campaigns can overstate the level of risk and requiring trans people to live without life-saving medication can also be a serious source of harm. It can also be cheaper to go black market than going private, and the only option in countries without a legal pathway.
Treating yourself
At this stage, I'm ready to say you're probably better off doing this than relying on your doctor. Gender doctors are notoriously hopeless, and will arbitrarily muck up your dose, refuse to experiment, be years behind best practice, find reasons to deny care...they also disempower, causing you to invest false hope in their competence which can be more dangerous. You'll need to be doing your own research anyway.
And, of course, discussions of the danger of self-medicating do not take into account the dangers of being unmedicated, which are considerable. Not just death, but surviving in a grey and hollow wasteland of unlife.
The concept of just dosing yourself with something is scary, but in practice you'd have to be pretty unlucky for taking hormones to make you so ill it is an immediate emergency. It does happen occasionally, but I've never heard of it. Problems on T build up over time. It's also very rare for people to be taken off T entirely for health reasons (I've lurked trans communities for over a decade now, and I think I know a single case.) Look at the health guides, and look up the medication leaflet online for the substance you're about to take: these will list 'Don't Take If' and 'Take Caution If' for T. If you are in those categories, then you're the sort of person for whom the actual health safety of being your own doctor is a concern.
It's important to get regular blood tests on T, because it can cause difficulty with your liver - but these problems build up slowly over time. Make sure you've budgeted for blood tests: your GP may agree to do them as a harm reduction measure, or you may have to order a private service blood test. Every three months initially is a good pattern.
Alternatives to self-medicating
If you're able to go private, look into it. Maybe there is a local mutual aid who can help you fund treatment?
If you are in the UK, at least try to get a bridging prescription.
If you intend to go on 'low dose T', you might want to consider going to your GP in the guise of a woman suffering from low libido or menopause. Tell them you're experiencing sexual intimacy problems with your husband and, as such, cannot feel fully fulfilled as a complete woman. Such testosterone prescriptions are more quickly given, because our society is a trashfire.
The Law in the UK
It is extremely unlikely you will get into trouble for self-medicating T.
Cops 101
It's important to know your rights because police will frequently lie or misrepresent the law to get you to incriminate yourself in some way. The basic advice is to say absolutely nothing and keep stonewalling any kind of information until you're released. Be uncooperative.
- Stop & Search: what to do if stopped and searched by the police
- Arrest: what to do if arrested and taken to the station
- Do not invite them into your house - like vampires, the police cannot just come in without permission. Just like in the movies, the police need to come with a warrant for the specific thing they suspect you of (but can sieze other evidence of other crimes once they're in) unless it's an emergency (for example, they can hear someone shouting for help). If they have the warrant, they can use reasonable force to enter the property.
Testosterone is an anabolic steroid - a Class C drug, under the Misuse of Drugs Act 1971.
These things count as crime:
- it is illegal to manufacture, supply or possess/import/export steroids with the intent to supply, without a licence to do so. The maximum penalty for these offences is 14 years in prison and/or a heavy fine
- It's worth emphasising that giving some meds to a buddy DOES count as 'supply' or 'attempt to supply'
- As of 2012, it is illegal to import steroids by ordering them through mail order or online and having them delivered to you from outside the UK.
These things are not a Crime
- Posessing steroids: there is no offense if you posess steroids. Class C drugs can have a penalty up to 2 years’ imprisonment and/or an unlimited fine, but this does not apply to Image and Performance Enhancing Drugs.
- By implication, ordering steroids from within the UK is probably not a crime
- Under the Misuse of Drugs act 1971, it is not an offense to supply needles and syringes - even if you know or suspect they might be used to take illegal drugs with. It IS a crime to supply (or offer to supply) other kinds of drugtaking paraphenalia, although in practice it's now unheard of for people to be arrested for this (which is why there are high street headshops with bongs fully on display). It's likely that you might be prosecuted for this if the police couldn't nab you for what they really wanted to (i.e. they can't prove you're selling actual drugs, but they can get you for this)
- Implicitly, it seems unlikely that merely owning syringes, needles etc is a crime
Studies & Science
I'm curious to learn more about the specifics of different T preparations and methods, esp in terms of varying results. As far as I can tell, the assumption is that they're identical - they produce some masculinisation which is presumed to be what all transmasculine people ultimately want. But they don't - we're individuals - and so I'm interested to learn what, if anything, we can do to customise our outcomes more
All of these studies are of cis men, unless otherwise stated; some are cis men with particular conditions, or who are elderly, or part of particular groups. This may or may not be applicable to us. At the level I'm capable of, I can't say whether these impact transmasc people significantly or at all - but they are interesting, let's say. Experiment with as you wish.
- SQ is an acceptable alternative to IM and most people prefer it
- IM injections increase hematocrit more than gel
- T Undecanoate every 12 weeks vs T Enanthate every 3 weeks? More or less the same in terms of outcome.
- Can you administer T Undecanoate with SQ? Yes, but it might hurt more 24 hours afterwards
- Taking T influences the structure of the brain, particularly parts researchers believe are involved in depression...but those same brain structures do NOT change in trans women taking estrogen; in other words, they've observed testosterone treatment improving our lives, but estrogen treatment not making trans women's lives worse. The researchers seem not to have come to the obvious conclusions here.
- Transition should not impact your sense of smell (but it did mine anyway)
- At least some of the research on T is being funded by the military to investigate increased effectiveness in soldiers. Grim!
- There's some evidence that fenugreek really does do something around testosterone, albeit - like all suppliments - difficult to measure how much and safely. Fenugreek seeds were discovered in King Tut's tomb, mentioned in early Jewish texts, and are an ingredient in Indian and Middle Eastern foods.
- A study following FtMs on T for 18.5 years discovered there was no increase in death compared to the normal population. That's good to know for people fearmongering about T; but notice the bloodcurdling situation for trans women, whose mortality was 51% higher than the average. Eek.
- There is little to no studies on the impact of testosterone on mood and wellbeing, in either cis men or trans men. All studies focus on how fast physical masculinisation occurs.
Studies I'd like to see
- Does DHT cream increase penis length for trans men?
- Does HGC increase penis length for trans men?
- Does pumping increase penis length for trans men?
- What is the relationship between T and dreaming? Why did my trauma nightmares stop?
- Why do some people need different doses than others? Can we work it out in advance?
- Any research on the psychological side effects of endocrine dysphoria - in cis or trans men?
Non-Hormone Tips
Other links, as and when I run across them
Weightlifting
The FTM's Complete Guide to Looking Like a Hot Dude - specifically recommended for the section on weight training! But the clothing guide is also very good. Note that this guide discusses (and advises) weight loss.
There's also a community reddit: r/FtmFitness
Vocal Training
Transmasc Voice Guide - vocal training is one of these things often associated with trans women & only (occasionally!) funded for trans women in the UK on the basis that T drops your voice anyway. But you might not want to be on T/or, it might not do the trick.
Plus a Discord Community; and there's a reddit for voice with a transmasc tag; and look on youtube for videos
Vocal surgery exists and works, but is not widely available.
Singing
A common worry! Here's a study on the Singing Voice In The First 2 Years Of T by Tessa Romano, a singing tutor; and there's a lot of resources here.
Plus my own section on this, on Karaoke
Hair Growth
I Will Teach You To Be Hairy - community-made guide to growing hair while not on T. Author intends to update soon, as putting hairdye on newly grown hair can cause them to burn and you shouldn't.
What about preventing hair loss? There's community rumblings about minoxidil, dermarollers, and topical finasteride (the latter can counteract your progress from T so...it's a fine art). Basically, people are experimenting with these but I've not done any real research: ask about.
Poesil's Facial Hair and Bearding Infodump
On microneedling for preventing hair loss, A Randomized Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study
Top Surgery
- High BMI as risk factor in mastectomy in transmasculine individuals: a retrospective matched case-control study - suggests the risk is higher in some patients, but comes to the conclusion that this means patients must be given more information so they can make a free choice, NOT that surgery ought to be barred
Dicks
Why yes, there are absolutely people researching how to get more length without surgery. You can visit r/growyourTdick, or the sister sub r/GrowYourClit for ideas.
- Using a special T cream (different from the gel!) can provide bottom growth even if you're not using HRT overall; there's mixed reports as to whether doing this and HRT will cause it to grow more or faster. It contains DHT and must be prepared by a compounding pharmacy. This works in cis boys with slow growth for intersex reasons, but there have been no studies in us. DHT cream is extremely hard to get your hands on. The primary information sources on DHT for trans men are this article, this tumblr and posts on this blog. One person who supposedly offers it is the controversial Dr Will Powers. All told, the evidence is not there either way because the research has not been done: it's possible that the extra growth people experience they were going to have anyway.
- This user has, rather brilliantly, been using AMAB foreskin restoration resources, like this, to stretch out his foreskin for a more sensitive head and more 'natural' look.
- Pumping is an option for play, that some believe also leads to more girth over time.
- If you're window-shopping for silicone, there's reviews and discussion at r/transmascdicks.
- Queer Mushroom Forest has a great guide to stroker toys, making your own packer harness, and other trans 'intimate wellness' topics. Really beautiful website design too.
Healthcare
- Ben Haseen's guide to chest self-examination to avoid breast cancer: pdf and video
Changelog
March 2026
- created an index
- Previous documented update dates: 15/5/2023, 20/11/2025